一点思考。这是一个有争议的研究领域,有许多互相矛盾的结果,目前尚无定论。这方面的讨论和影响非常复杂,比如此类结果给了跨性别合法性和去病化的依据,因此对改善群体医疗状况有相当大的意义;但另一方面,对自由意志、社会建构等是一个不利的证据,也阻碍了去性别化、拒绝性别标签与特质绑定这方面的主张推行。
我长时间以来会害怕这个结果真的成为铁证,不是因为“它能断言我不是女性或者不能成为女性”,就好像如果我不是青蛙,我也不会有成为青蛙的强烈愿望。我更多恐惧的是,“我没有掌握某些‘性别天赋’的可能——我是残次品”,以及“根据性别划分出圈层非常合理——我会被某些群体拒绝和排斥”。这相当于性别本质主义重新给我套上锁链,而这种焦虑需要通过正面的理论解析和实践尝试来破解而非绕过,否则依然很难建立自我认同和自我接纳,也无法治愈社交自信上的一道巨大创伤。
18 个赞
“correlation doesn’t means causation”
10 个赞
的确,背后的具体逻辑关系很可能相当错综复杂
所以现在还是以脚踏实地改变自己为主
4 个赞
那个,虽然我无权干涉你发什么内容
但是在我的帖子回复我明显无法理解的信息,我会困扰的
2 个赞
居然能在这里看到楼子哥我好欣慰呜呜呜x
3 个赞
刚才加他们群了,群聊的结果比较失望
2 个赞
他们那个群确实……楼子哥一百多粉的时候我进去的,时间长了感觉群里气氛很怪我就出来了……就 别的vup群我也加了,都没有那种我看不懂/不理解/没法加入的感觉x
1 个赞
确实说话不是很能对得上节奏,我也暂时收群助手了
不过与孟哥本人对话好像没什么问题,普通的好人(
1 个赞
感谢查阅原文!所以这个方面的结果确实非常有争议
还有下次记得,图片和文字之间留一个回车,最好现在也编辑一下
4 个赞
好的谢谢提醒,已更改
1 个赞
谢谢~辛苦啦
1 个赞
那普通的男女大脑…不是也有差异吗。。。
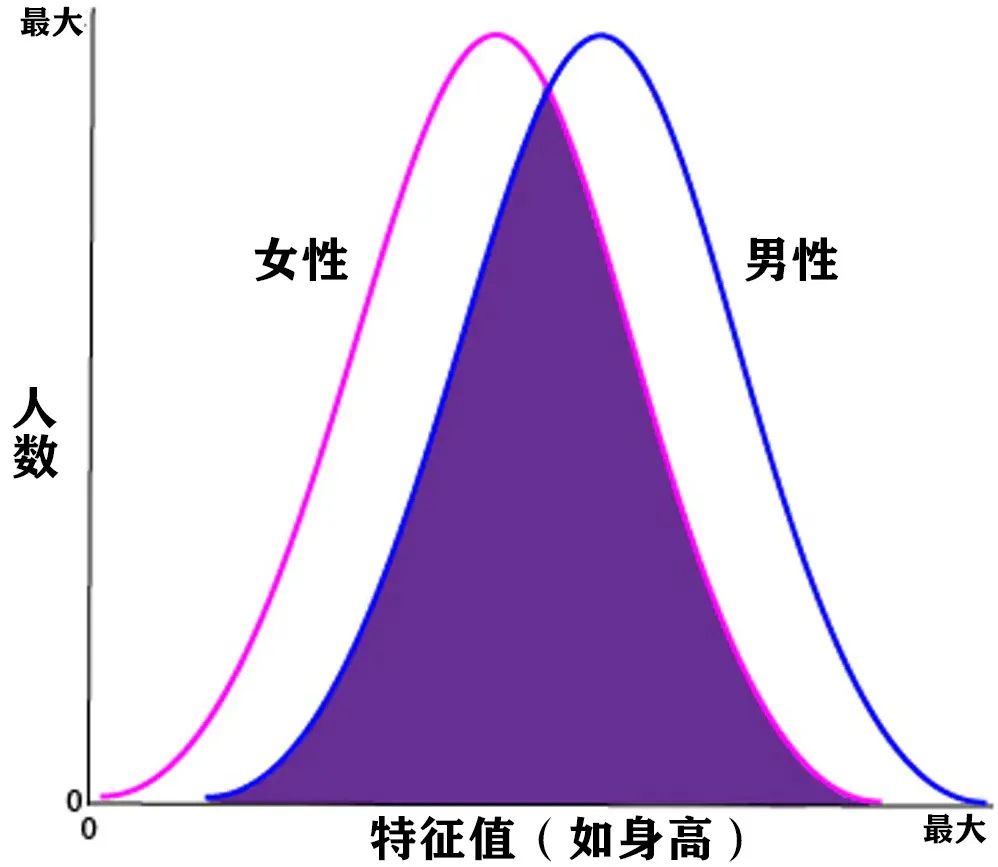
就算有,那种统计学上的规律在个体上可能……没那么大影响的!
“就好像大脑性别差异,当你以为是大脑差异就是导致男孩喜欢蓝色,女孩喜欢粉色的时候,你其实就已经偏离了科学的道路了——神经学只是强调了差异,但是还没能解释这些差异与行为的关系 。”
原文链接https://www.zhihu.com/answer/1455626191
好了,神经科学现在还没有那么强,给不出什么有实际意义的判断
5 个赞
所以之前我就在想一个很危险的命题
“人的性别是钉死的不能自己决定,只不过判断标准从生殖器变成大脑结构”
根据和大家的讨论,这个命题应该是错的,谢谢~
6 个赞
小时候就觉得粉色挺好看的,然后因为说小女孩才喜欢,所以强迫自己把这部分藏了下去,喜欢蓝色,不过也是那种比较浅的,天蓝之类的
现在放开了,粉色和蓝色都超棒!粉蓝超好看!
9 个赞
吃药会改变认知功能
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6719479/
The brain and cognition
Recent studies have investigated baseline differences between the brains of trans versus cis individuals as well as the effect of GAHT on the brain and cognition. The white matter microstructure of TW prior to initiation of GAHT has been characterized by diffusion tensor imaging to be between control females and control males.222–225 Hahn and colleagues226 also described different structural connectivity networks in 21 TW prior to initiating GAHT compared with control females and males. Seiger and colleagues227 analyzed brain MRIs of 14 TW (mean age 26.9 ± 6.1 years) at baseline and after at least 4 months (169 days ± SD 38 days) of continuous oral or transdermal oestradiol and anti-androgens (cyproterone acetate ± GnRHa ± finasteride) and found decreases in the hippocampal region, increases in the ventricles and a correlation between progesterone levels and changes in grey matter structure. Mueller and colleagues228 found neuroanatomical volume differences in the amygdala, putamen and corpus callosum in TW compared with cis women but not cis men, suggesting the possibility of localized influence of sex hormones on neuroanatomy. These studies suggest there are hormonal influences on cortical and subcortical structures related to cognition, memory and emotional processing. Reviews stress that additional short- and long-term studies are needed to better understand the role of sex hormones on the adult human brain structure and function and how they relate to psychological differences between females and males.229,230
Brain-derived neurotrophic factor (BDNF) is involved in neurogenesis, neuronal maturation and synaptogenesis, influencing brain plasticity. A study of 10 TW from Belgium showed a significant decrease in BDNF levels after 12 months of GAHT (p = 0.014) independent of age, weight, BMI, total fat mass, total lean mass, LH, FSH, oestradiol, testosterone, cortisol, physical activity or smoking.231 Therefore, it was concluded that the decreased BDNF in TW after GAHT resulted from the GAHT rather than as a consequence of or risk factor for gender identity.231
Nguyen and colleagues232 published a recent review of cross-sectional and longitudinal studies from the last 5 years, nearly all from European cohorts, and summarized fewer depressive symptoms, anxiety, problems with socialization and interpersonal functioning, global functional impairment, interpersonal sensitivity and hostility in TW on GAHT compared with baseline. They also summarized the general findings above that GAHT is correlated with changes in global and regional brain volumes, white matter microstructure and in cognitive performance on sex-biased tasks requiring verbal and visual memory in the direction of gender identity rather than assigned sex.232 However, no studies have examined how GAHT influences executive function and cognitive domains used for daily living, and additional research will provide valuable data on these and other brain processes.
4 个赞
https://en.wikipedia.org/wiki/Causes_of_transsexuality#Brain_structure
Brain structure
General
Several studies have found a correlation between gender identity and brain structure.[8] A first-of-its-kind study by Zhou et al. (1995) found that in a region of the brain called the bed nucleus of the stria terminalis (BSTc), a region which is known for sex and anxiety responses (and which is affected by prenatal androgens),[9] cadavers of six persons who were described as having been male-to-female transsexual or transgender persons in life had female-normal BSTc size, similar to the study’s cadavers of cisgender women. While those identified as transsexual had taken hormones, this was accounted for by including cadavers of non-transsexual male and female controls who, for a variety of medical reasons, had experienced hormone reversal. The controls still had sizes typical for their gender. No relationship to sexual orientation was found.[10]
In a follow-up study, Kruijver et al. (2000) looked at the number of neurons in BSTc instead of volumes. They found the same results as Zhou et al. (1995), but with even more dramatic differences. One MtF subject, who had never gone on hormones, was also included and matched up with the female neuron counts nonetheless.[11]
In 2002, a follow-up study by Chung et al. found that significant sexual dimorphism (variation between sexes) in BSTc did not become established until adulthood. Chung et al. theorized that either changes in fetal hormone levels produce changes in BSTc synaptic density, neuronal activity, or neurochemical content which later lead to size and neuron count changes in BSTc, or that the size of BSTc is affected by the generation of a gender identity inconsistent with one’s assigned sex.[12]
It has been suggested that the BSTc differences may be due to the effects of hormone replacement therapy. It has also been suggested that because pedophilic offenders have also been found to have a reduced BSTc, a feminine BSTc may be a marker for paraphilias rather than transsexuality.[2]
In a review of the evidence in 2006, Gooren considered the earlier research as supporting the concept of transsexuality as a sexual differentiation disorder of the sex dimorphic brain.[13] Dick Swaab (2004) concurs.[14]
In 2008, a new region with properties similar to that of BSTc in regards to transsexuality was found by Garcia-Falgueras and Swaab: the interstitial nucleus of the anterior hypothalamus (INAH3), part of the hypothalamic uncinate nucleus. The same method of controlling for hormone usage was used as in Zhou et al. (1995) and Kruijver et al. (2000). The differences were even more pronounced than with BSTc; control males averaged 1.9 times the volume and 2.3 times the neurons as control females, yet regardless of hormone exposure, MtF transsexuals were within the female range and the FtM transsexual within the male range.[15]
A 2009 MRI study by Luders et al. of 24 MtF transsexuals not yet treated with cross-sex hormones found that regional gray matter concentrations were more similar to those of cisgender men than to those of cisgender women, but there was a significantly larger volume of gray matter in the right putamen compared to cisgender men. Like earlier studies, it concluded that transsexuality was associated with a distinct cerebral pattern.[16] (MRI allows easier study of larger brain structures, but independent nuclei are not visible due to lack of contrast between different neurological tissue types, hence other studies on e.g. BSTc were done by dissecting brains post-mortem.)
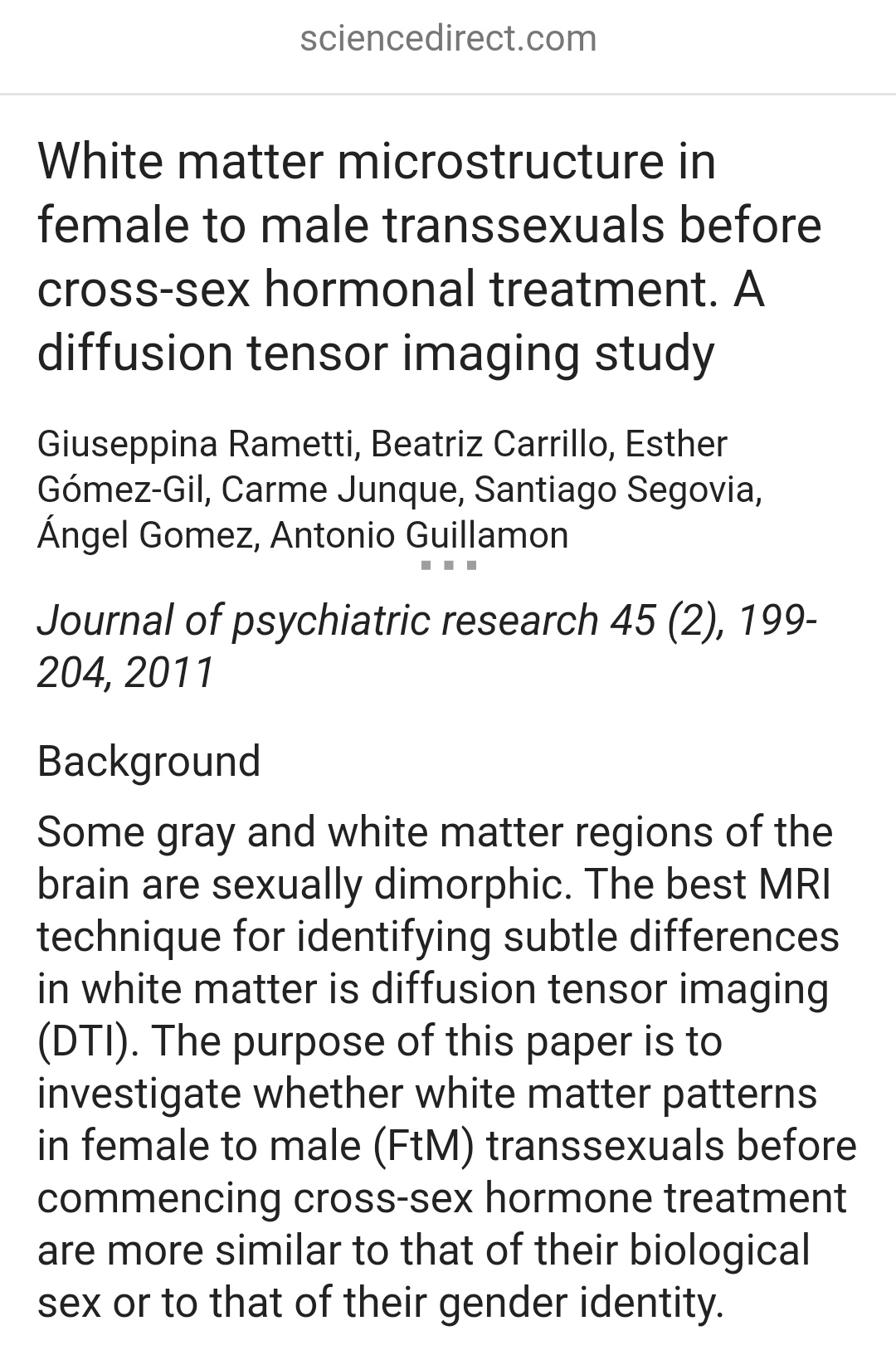
An additional feature was studied comparing 18 female-to-male transsexuals who had not yet received cross-sex hormones with 24 cisgender male and 19 female gynephilic controls, using an MRI technique called diffusion tensor imaging or DTI.[17] DTI is a specialized technique for visualizing white matter of the brain, and white matter structure is one of the differences in neuroanatomy between men and women. The study took into account fractional anisotropy values for white matter in the medial and posterior parts of the right superior longitudinal fasciculus (SLF), the forceps minor, and the corticospinal tract. Rametti et al. (2010) discovered that, “Compared to control females, FtM showed higher FA values in posterior part of the right SLF, the forceps minor and corticospinal tract. Compared to control males, FtM showed only lower FA values in the corticospinal tract.”[17] The white matter pattern in female-to-male transsexuals was found to be shifted in the direction of biological males.
Hulshoff Pol et al. (2006) studied the gross brain volume of 8 male-to-female transsexuals and in six female-to-male transsexuals undergoing hormone treatment. They found that hormones changed the sizes of the hypothalamus in a gender consistent manner: treatment with male hormones shifted the hypothalamus towards the male direction in the same way as in male controls, and treatment with female hormones shifted the hypothalamus towards the female direction in the same way as female controls. They concluded: “The findings suggest that, throughout life, gonadal hormones remain essential for maintaining aspects of sex-specific differences in the human brain.”[18]
A 2016 review agreed with the other reviews when considering androphilic trans women and gynephilic trans men. It reported that hormone treatment may have large effects on the brain, and that cortical thickness, which is generally thicker in cisgender women’s brains than in cisgender men’s brains, may also be thicker in trans women’s brains, but is present in a different location to cisgender women’s brains.[2] It also stated that for both trans women and trans men, “cross-sex hormone treatment affects the gross morphology as well as the white matter microstructure of the brain. Changes are to be expected when hormones reach the brain in pharmacological doses. Consequently, one cannot take hormone-treated transsexual brain patterns as evidence of the transsexual brain phenotype because the treatment alters brain morphology and obscures the pre-treatment brain pattern.”[2]
Androphilic male-to-female transsexuals
Studies have shown that androphilic male-to-female transsexuals show a shift towards the female direction in brain anatomy. In 2009, a German team of radiologists led by Gizewski compared 12 androphilic transsexuals with 12 cisgender males and 12 cisgender females. Using functional magnetic resonance imaging (fMRI), they found that when shown erotica, the cisgender men responded in several brain regions that the cisgender women did not, and that the sample of androphilic transsexuals was shifted towards the female direction in brain responses.[19]
In another study, Rametti and colleagues used diffusion tensor imaging (DTI) to compare 18 androphilic male-to-female transsexuals with 19 gynephilic males and 19 androphilic cisgender females. The androphilic transsexuals differed from both control groups in multiple brain areas, including the superior longitudinal fasciculus, the right anterior cingulum, the right forceps minor, and the right corticospinal tract. The study authors concluded that androphilic transsexuals were halfway between the patterns exhibited by male and female controls.[20]
A 2016 review reported that early-onset androphilic transgender women have a brain structure similar to cisgender women’s and unlike cisgender men’s, but that they have their own brain phenotype.[2]
Gynephilic male-to-female transsexuals
Research on gynephilic trans women is considerably limited.[2] While MRI taken on gynephilic male-to-female transsexuals have likewise shown differences in the brain from non-transsexuals, no feminization of the brain’s structure have been identified.[2] Neuroscientists Ivanka Savic and Stefan Arver at the Karolinska Institute used MRI to compare 24 gynephilic male-to-female transsexuals with 24 cisgender male and 24 cisgender female controls. None of the study participants were on hormone treatment. The researchers found sex-typical differentiation between the MtF transsexuals and cisgender males, and the cisgender females; but the gynephilic transsexuals “displayed also singular features and differed from both control groups by having reduced thalamus and putamen volumes and elevated GM volumes in the right insular and inferior frontal cortex and an area covering the right angular gyrus”.[21]
The researchers concluded that:
Contrary to the primary hypothesis, no sex-atypical features with signs of ‘feminization’ were detected in the transsexual group … The present study does not support the dogma that [male-to-female transsexuals] have atypical sex dimorphism in the brain but confirms the previously reported sex differences. The observed differences between MtF-TR and controls raise the question as to whether gender dysphoria may be associated with changes in multiple structures and involve a network (rather than a single nodal area).[21]
Berglund et al. (2008) tested the response of gynephilic MtF transsexuals to two steroids hypothesized to be sex pheromones: the progestin-like 4,16-androstadien-3-one (AND) and the estrogen-like 1,3,5(10),16-tetraen-3-ol (EST). Despite the difference in sexual orientation, the MtFs’ hypothalamic networks activated in response to the AND pheromone, like the androphilic female control groups. Both groups experienced amygdala activation in response to EST. Gynephilic male control groups experienced hypothalamic activation in response to EST. However, the MtF subjects also experienced limited hypothalamic activation to EST. The researchers concluded that in terms of pheromone activation, MtFs occupy an intermediate position with predominantly female features.[22] The MtF transsexual subjects had not undergone any hormonal treatment at the time of the study, according to their own declaration beforehand, and confirmed by repeated tests of hormonal levels.[22]
A 2016 review reported that gynephilic trans women differ from both cisgender male and female controls in non-dimorphic brain areas.[2]
Gynephilic female-to-male transsexuals
Fewer studies have been performed on the brain structure of transgender men than on transgender women.[2] A team of neuroscientists, led by Nawata in Japan, used a technique called single-photon emission computed tomography (SPECT) to compare the regional cerebral blood flow (rCBF) of 11 gynephilic FtM transsexuals with that of 9 androphilic cis females. Although the study did not include a sample of biological males so that a conclusion of “male shift” could be made, the study did reveal that the gynephilic FtM transsexuals showed significant decrease in blood flow in the left anterior cingulate cortex and a significant increase in the right insula, two brain regions known to respond during sexual arousal.[23]
A 2016 review reported that the brain structure of early-onset gynephilic trans men generally corresponds to their assigned sex, but that they have their own phenotype with respect to cortical thickness, subcortical structures, and white matter microstructure, especially in the right hemisphere.[2] Morphological increments observed in the brains of trans men might be due to the anabolic effects of testosterone.[2]
Prenatal androgen exposure
Prenatal androgen exposure, the lack thereof, or poor sensitivity to prenatal androgens are commonly cited mechanisms to explain the above discoveries. To test this, studies have examined the differences between transsexual and cisgender individuals in digit ratio (a generally accepted marker for prenatal androgen exposure). A meta-analysis concluded that the effect sizes for this association were small or nonexistent.[24]
Congenital adrenal hyperplasia in persons with XX sex chromosomes results in what is considered to be excess exposure to prenatal androgens, resulting in masculinization of the genitalia and, typically, controversial prenatal hormone treatment[25] and postnatal surgical interventions.[26] Individuals with CAH are usually raised as girls and tend to have similar cognitive abilities to the typical female, including spatial ability, verbal ability, language lateralization, handedness and aggression. Research has shown that people with CAH and XX chromosomes will be more likely to be same sex attracted,[25] and at least 5.2% of these individuals develop serious gender dysphoria.[27]
In males with 5-alpha-reductase deficiency, conversion of testosterone to dihydrotestosterone is disrupted, decreasing the masculinization of genitalia. Individuals with this condition are typically raised as females due to their feminine appearance at a young age. However, more than half of males with this condition raised as females become males later in their life. Scientists speculate that the definition of masculine characteristics during puberty and the increased social status afforded to men are two possible motivations for a female-to-male transition.[27]
4 个赞
虽然不知道删除了什么,但是我得说
不要拿删除当隐藏用,删除就等于是不希望我看到哦
所以我不会点进去一个一个看的
1 个赞
Contrary to the primary hypothesis, no sex-atypical features with signs of ‘feminization’ were detected in the transsexual group … The present study does not support the dogma that [male-to-female transsexuals] have atypical sex dimorphism in the brain but confirms the previously reported sex differences. The observed differences between MtF-TR and controls raise the question as to whether gender dysphoria may be associated with changes in multiple structures and involve a network (rather than a single nodal area).
与最初的假设相反,在跨性别群体…中没有检测到有女性化迹象的性别非典型特征 。目前的研究并不支持[男性到跨性别女性]在大脑中存在非典型的性二态性的学说,但证实了之前报道的性别差异。观察到的MTF-TR和对照组之间的差异提出了一个问题,即性别焦虑是否可能与多个结构的变化有关,并涉及一个网络(而不是一个单一的结节区域)。
3 个赞
也就是说会有影响,但是并非简单的分界线,而是某种复杂模式的形成
1 个赞